Related
See More 


A staggering 24% of patients at hospital admission are found to be at risk for malnutrition, a factor linked to potential declines in physical and mental function, along with compromised clinical outcomes. This emphasises the vital role of medical nutrition (MN) in preventing further deterioration in clinical conditions and supporting recovery.
Over the years, MN products have become increasingly specialised to address unmet needs associated with specific diseases, such as Inflammatory Bowel Disease (IBD) and cancer. Yet, as patients become increasingly polymorbid, one must consider the sustainability of this condition-specific approach over the long term.
Malnutrition, or undernutrition, can be defined as "a state resulting from lack of intake or uptake of nutrition that leads to altered body composition (decreased fat-free mass) and body cell mass1. The risk for malnutrition in hospitals is especially pronounced among patients over 70 years old, and those with conditions such as cancer, cardiac diseases, respiratory diseases, and gastrointestinal (GI) diseases, as illustrated in Figure 1. Consequently, these patients commonly grapple with diminished physical and mental function, resulting in impaired clinical outcomes. Indeed, disease-caused malnutrition is associated with heightened susceptibility to infections and comorbidities, delayed wound healing, impaired recovery, diminished quality of life and an increased likelihood of mortality. These consequences extend beyond the individual, impacting healthcare systems with higher costs, longer hospital stays and increased treatment needs. Therefore, addressing malnutrition within the healthcare landscape remains critical.

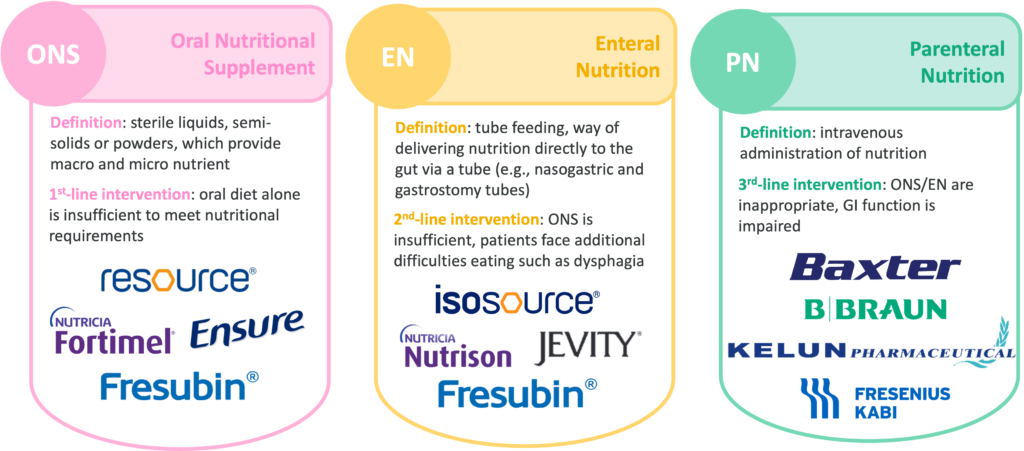
Dietary changes and MN are the main treatments for malnutrition, aiming to increase undernourished patients’ nutritional intake. Medical nutrition therapy, as defined by EU legislation, refers to “foods for special medical purposes”, i.e., “specially processed or formulated and intended for the dietary management of patients”3. This term encompasses oral nutritional supplements (ONS), enteral tube feeding (enteral nutrition (EN)) and parenteral (intravenous) nutrition (PN), further detailed in Figure 2. ONS is usually the preferred approach4, as it offers a non-invasive solution that can easily be initiated to enrich a patient’s diet. EN typically becomes a consideration if ONS proves insufficient or if patients face additional GI difficulties, such as dysphagia. PN tends to be reserved as a last resort for more critically ill patients who cannot receive nutrition orally and when EN is contraindicated, for instance, due to an impaired GI function or due to surgery. Initially, MN products were only indicated for general malnutrition and had simple formulas – high-calorie and/or high-protein solutions designed to provide a concentrated source of essential nutrients. These products were segmented by age group, product format (ONS vs EN) and flavours.
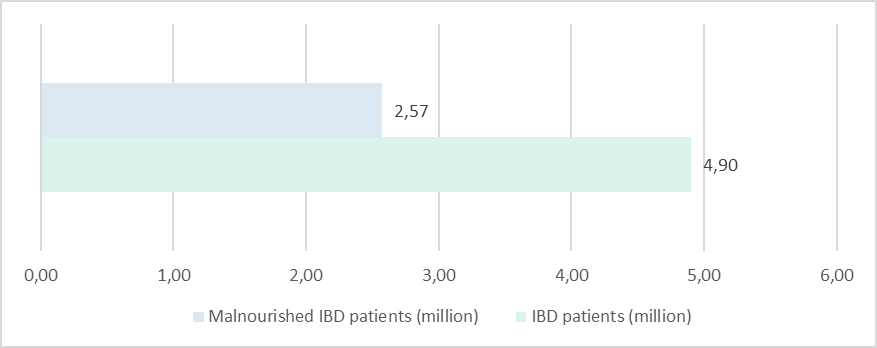
As an illustration, standard MN is recommended for Inflammatory Bowel Disease (IBD) due to the heightened risk of malnutrition associated with this condition. IBD encompasses Crohn’s Disease (CD) and Ulcerative Colitis, two chronic, relapsing, inflammatory disorders of the GI tract. This intestinal inflammation, combined with GI symptoms (e.g., severe diarrhoea, rectal bleeding) and certain medications (e.g., corticosteroids, sulfasalazine and methotrexate), can lead to complications that facilitate malnutrition. These complications include malabsorption, chronic blood and protein loss, and intestinal bacterial overgrowth. With a reported malnutrition prevalence ranging from 20% to 85%5,6, we estimate that 2.57m patients living with IBD worldwide may be malnourished as shown on Figure 3. Weight loss is particularly common in hospitalised IBD patients, reported in 70-80% of cases, and in 20-40% of CD outpatients7,8.
To effectively prevent and manage malnutrition in IBD patients, ESPEN guidelines recommend initiating a MN treatment with standard ONS9, such as Resource, Ensure or Fortimel. Patients often transition to standard EN, especially during the acute phase of CD or in remission to prevent relapse, as it has proven to be a highly effective therapy. Both ONS and EN standard solutions have demonstrated efficacy in addressing nutritional deficiencies despite symptoms (e.g., loss of appetite, nausea) and complications, thereby reducing the need for hospitalisation and surgery. Standard EN can even help heal the lining of the intestines, reduce swelling, and improve overall symptoms. Additionally, these have also been shown to prevent osteoporosis and paediatric development issues in these patients10.